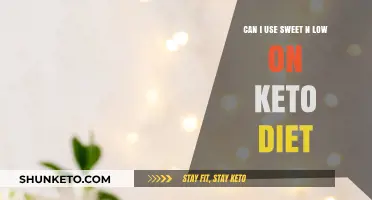
Insulin-dependent diabetics, particularly those with Type 1 diabetes, often face unique challenges when considering dietary changes, and the ketogenic (keto) diet is no exception. The keto diet, which is high in fats and low in carbohydrates, aims to shift the body into a state of ketosis, where it burns fat for energy instead of glucose. While this can be beneficial for weight loss and blood sugar control in some individuals, it poses specific risks for insulin-dependent diabetics. Fluctuations in blood sugar levels, the potential for diabetic ketoacidosis (DKA), and the need for precise insulin dosing make the keto diet a complex and potentially risky choice. However, with careful monitoring, medical supervision, and individualized adjustments, some insulin-dependent diabetics may be able to safely adopt a modified keto approach. Consulting with healthcare professionals, including endocrinologists and dietitians, is essential to ensure safety and efficacy.
| Characteristics | Values |
|---|---|
| Feasibility | Possible with strict monitoring and medical supervision |
| Blood Sugar Control | Improved stability due to reduced carbohydrate intake |
| Insulin Dosage | Often requires significant reduction to avoid hypoglycemia |
| Ketone Monitoring | Essential to prevent diabetic ketoacidosis (DKA) |
| Medical Supervision | Mandatory due to risks of hypoglycemia and DKA |
| Individual Variability | Outcomes vary based on individual health status and insulin sensitivity |
| Nutrient Balance | Requires careful planning to ensure adequate fiber, vitamins, and minerals |
| Long-Term Sustainability | May be challenging due to dietary restrictions and monitoring demands |
| Potential Benefits | Weight loss, improved HbA1c levels, reduced insulin resistance |
| Potential Risks | Hypoglycemia, DKA, electrolyte imbalances, and nutritional deficiencies |
| Recommended Approach | Gradual transition, frequent blood glucose checks, and regular consultations with healthcare providers |
Explore related products





What You'll Learn
![]()
Keto safety for Type 1 diabetics
Type 1 diabetics on a keto diet face unique risks due to their reliance on exogenous insulin and the diet’s inherent low-carb nature. The primary concern is hypoglycemia, as drastically reducing carbohydrate intake lowers blood glucose levels, requiring precise insulin dose adjustments. A study in *Diabetes Therapy* (2018) found that 45% of Type 1 participants on keto experienced hypoglycemic episodes within the first month, despite reducing basal insulin by an average of 20%. This highlights the need for vigilant monitoring and collaboration with a healthcare provider to fine-tune insulin regimens.
Implementing keto safely for Type 1 diabetics involves structured steps to mitigate risks. Start by gradually reducing carbohydrate intake over 2–3 weeks, monitoring blood glucose levels every 2–3 hours. Simultaneously, decrease basal insulin doses by 10–20% under medical supervision. Bolus insulin for protein and fat becomes critical, as these macronutrients can elevate blood glucose. Use a ratio of 1 unit of insulin for every 10–15 grams of protein and adjust based on post-meal readings. Continuous glucose monitoring (CGM) systems are invaluable for real-time data, allowing for swift corrections.
A comparative analysis of keto versus traditional low-fat diets for Type 1 diabetics reveals distinct advantages and challenges. Keto often improves HbA1c levels and reduces glycemic variability, as shown in a *JAMA* study (2020). However, the risk of diabetic ketoacidosis (DKA) increases if insulin doses are not appropriately reduced. In contrast, low-fat diets provide more flexibility in insulin management but may lead to higher post-meal glucose spikes. Keto’s strict macronutrient ratios demand discipline and education, making it less suitable for children or those with limited access to medical care.
Practical tips can enhance safety and adherence for Type 1 diabetics on keto. Always carry fast-acting glucose sources like juice or tablets to treat hypoglycemia promptly. Log all meals, insulin doses, and blood glucose readings to identify patterns and adjust protocols. Stay hydrated, as keto can increase fluid and electrolyte loss, which is particularly important for preventing DKA. Finally, prioritize regular consultations with an endocrinologist or dietitian to ensure the diet aligns with long-term health goals. Keto is not a one-size-fits-all solution but can be a viable option with careful planning and monitoring.
Navy SEALs and Keto: Unveiling Their High-Performance Diet Secrets
You may want to see also
Explore related products






![]()
Managing blood sugar on keto
Insulin-dependent diabetics often face unique challenges when considering a ketogenic diet, but with careful management, it can be a viable option. The keto diet, characterized by low carbohydrate intake and high fat consumption, naturally reduces blood sugar spikes, which can be beneficial for diabetics. However, the key to success lies in meticulous monitoring and adjustments to insulin dosages. For instance, as carbohydrate intake decreases, basal insulin needs may drop significantly, often by 30-50%, to prevent hypoglycemia. This requires frequent blood glucose checks, especially during the initial weeks of transitioning to keto.
One practical strategy for managing blood sugar on keto is to focus on consistent meal timing and portion control. Since fat becomes the primary energy source, meals should be balanced with moderate protein and high-quality fats like avocados, nuts, and olive oil. Carbohydrates should be limited to 20-50 grams per day, depending on individual tolerance. For example, a 45-year-old insulin-dependent diabetic might start with 20 grams of carbs daily, gradually increasing if blood sugar remains stable. Pairing carbs with fiber-rich foods, such as non-starchy vegetables, can further stabilize glucose levels by slowing digestion.
A critical aspect of keto for diabetics is understanding the role of protein in blood sugar management. While protein is essential, excessive intake can trigger gluconeogenesis, where the body converts protein into glucose, potentially raising blood sugar. To mitigate this, diabetics should aim for 0.8-1.2 grams of protein per kilogram of body weight daily. For a 70 kg individual, this translates to 56-84 grams of protein per day. Regularly testing blood glucose post-meals can help identify how specific protein sources affect individual responses.
Despite its benefits, the keto diet is not without risks for insulin-dependent diabetics. Hypoglycemia is a significant concern, particularly during the initial phase when insulin dosages are being adjusted. Symptoms like shakiness, confusion, or sweating require immediate treatment with fast-acting glucose. Additionally, ketoacidosis, a condition where ketone levels become dangerously high, is a risk if insulin doses are not properly calibrated. Continuous glucose monitoring (CGM) systems can be invaluable tools for real-time tracking, allowing for swift interventions when needed.
In conclusion, managing blood sugar on a keto diet for insulin-dependent diabetics requires a proactive and personalized approach. Success hinges on regular monitoring, precise insulin adjustments, and a well-structured meal plan. While the diet can improve glycemic control and reduce insulin needs, it demands vigilance to avoid complications. Consulting with a healthcare provider or endocrinologist is essential before starting keto, ensuring a safe and effective transition. With the right strategies, diabetics can harness the benefits of keto while maintaining stable blood sugar levels.
Is V8 Juice Keto-Friendly? A Guide to Low-Carb Juicing
You may want to see also
Explore related products






![]()
Insulin adjustments on keto
Insulin-dependent diabetics embarking on a keto diet must prioritize meticulous insulin adjustments to avoid hypoglycemia. The drastic reduction in carbohydrate intake—often below 50 grams daily—significantly lowers blood glucose levels, reducing the need for exogenous insulin. For instance, a Type 1 diabetic on a standard diet might require 1 unit of insulin per 10 grams of carbs, but on keto, this ratio becomes nearly obsolete. Immediate reductions in basal insulin (e.g., long-acting insulin like Lantus) by 10–20% are often necessary within the first 24–48 hours, followed by close monitoring of glucose levels every 2–3 hours. Failure to adjust promptly can lead to dangerous lows, especially during the initial transition phase.
The interplay between insulin and ketones adds another layer of complexity. Ketones, produced during fat metabolism on keto, can falsely elevate blood glucose readings on some meters, leading to over-treatment with insulin. To avoid this, diabetics should use meters that differentiate between glucose and ketones, such as the Abbott Libre Sense. Additionally, ketones themselves can blunt the body’s insulin sensitivity, requiring further fine-tuning of bolus doses. For example, a pre-meal bolus might need to be reduced by 20–30% initially, with adjustments based on post-meal glucose readings. Continuous glucose monitoring (CGM) systems become indispensable tools for real-time data, allowing for precise insulin titration.
Practical tips for insulin adjustment include starting with conservative reductions and gradually refining doses based on trends. For basal insulin, a 10% reduction can be implemented initially, with further 5% decrements every 2–3 days as needed. Bolus insulin should be halved for the first few meals, with subsequent doses guided by carbohydrate content (if any) and protein intake, as protein can still trigger a glucose response. For instance, a meal with 30 grams of protein might require 1–2 units of insulin, depending on individual sensitivity. Keeping a detailed log of insulin doses, meals, and glucose readings is critical for identifying patterns and making informed adjustments.
Caution must be exercised in older adults or those with renal impairment, as keto’s diuretic effect can exacerbate dehydration, altering insulin absorption and glucose dynamics. These individuals may require smaller, more frequent adjustments and closer monitoring. Similarly, diabetics on hybrid closed-loop systems (e.g., Tandem Control-IQ) should work closely with their endocrinologist to recalibrate settings, as the algorithm may not account for keto’s unique metabolic shifts. Regular communication with a healthcare team is non-negotiable, as keto’s impact on insulin needs can vary widely based on age, activity level, and comorbidities.
Ultimately, insulin adjustments on keto are a dynamic, patient-specific process requiring vigilance and adaptability. Success hinges on understanding the diet’s immediate and long-term effects on glucose metabolism, leveraging technology for real-time data, and maintaining open dialogue with healthcare providers. While the keto diet can offer glycemic benefits for insulin-dependent diabetics, it demands a proactive approach to insulin management to ensure safety and efficacy. With careful planning and monitoring, many find a stable balance that minimizes hypoglycemic risk while optimizing metabolic health.
Can You Do Keto Sometimes? Flexibility in Low-Carb Eating Explained
You may want to see also
Explore related products






![]()
Risks of ketoacidosis
Insulin-dependent diabetics considering the keto diet must be acutely aware of the heightened risk of diabetic ketoacidosis (DKA), a life-threatening condition. DKA occurs when the body produces excessive ketones due to a lack of insulin, leading to a dangerous metabolic imbalance. For those on a keto diet, the body is already in a state of ketosis, producing ketones as an alternative energy source. However, in insulin-dependent individuals, this process can spiral out of control, as insulin is crucial for regulating ketone production and preventing their excessive buildup.
Understanding the Mechanism
When insulin levels are insufficient, the body breaks down fat at an accelerated rate, releasing ketones into the bloodstream. In a non-diabetic individual or someone with well-managed diabetes, insulin keeps ketone levels in check. For insulin-dependent diabetics, particularly Type 1, the absence of endogenous insulin means ketones can accumulate rapidly, leading to DKA. Symptoms include nausea, vomiting, abdominal pain, rapid breathing, and confusion. If left untreated, DKA can result in coma or death. The keto diet, while low-carb, does not inherently cause DKA, but it requires meticulous insulin management to avoid this risk.
Practical Precautions
To mitigate the risk of DKA, insulin-dependent diabetics on a keto diet must monitor blood glucose and ketone levels multiple times daily. Ketone testing can be done via urine strips, blood meters, or breath analyzers. Aim to keep blood ketone levels below 0.6 mmol/L. Adjust insulin dosages as needed, particularly during meals, to account for dietary changes. Consult an endocrinologist or dietitian to create a personalized insulin plan. Additionally, stay hydrated, as dehydration can exacerbate ketone production. Avoid starting the keto diet during periods of illness or stress, as these conditions increase the risk of DKA.
Comparative Risks and Benefits
While the keto diet may improve blood sugar control and reduce insulin requirements in some diabetics, the risk of DKA cannot be overlooked. For Type 1 diabetics, the diet’s strict carbohydrate restriction may lead to unpredictable glucose fluctuations, making insulin dosing challenging. Type 2 diabetics on insulin may fare better but still require close monitoring. Compared to other diets, keto’s emphasis on fat and protein can be beneficial for weight management and glycemic control, but it demands a higher level of vigilance. The decision to adopt keto should be weighed against individual health status, lifestyle, and ability to manage diabetes rigorously.
Emergency Preparedness
Despite precautions, the risk of DKA is never zero. Insulin-dependent diabetics on keto must have a clear action plan for emergencies. Keep a supply of fast-acting insulin and glucose tablets on hand. If ketone levels rise above 1.5 mmol/L, increase fluid intake and administer insulin as directed by a healthcare provider. Seek immediate medical attention if symptoms of DKA appear. Educate family members or close contacts about DKA signs and emergency protocols. Regular follow-ups with a healthcare team are essential to assess the diet’s impact on metabolic health and adjust strategies accordingly.
In conclusion, while the keto diet is not inherently off-limits for insulin-dependent diabetics, it demands a high degree of caution and preparation. The risk of ketoacidosis is a critical consideration that requires proactive management, from rigorous monitoring to emergency readiness. With the right approach, some individuals may safely adopt keto, but it is not a one-size-fits-all solution. Always prioritize medical guidance and individualized care in navigating this dietary choice.
Melatonin and Keto: Can You Safely Combine the Two?
You may want to see also
Explore related products






![]()
Nutrient needs for diabetics on keto
Insulin-dependent diabetics considering the keto diet must prioritize nutrient needs to maintain metabolic balance and prevent complications. The keto diet’s high-fat, low-carbohydrate structure can alter nutrient absorption and utilization, requiring careful adjustments for this population. For example, fat-soluble vitamins (A, D, E, K) become critical due to increased fat intake, while electrolyte imbalances (sodium, potassium, magnesium) are common early on, necessitating supplementation or dietary sources like avocados, spinach, and nuts. Monitoring these nutrients ensures the diet supports rather than undermines health.
Analyzing macronutrient ratios reveals the keto diet’s unique demands for diabetics. Typically, keto involves 70-75% fat, 20-25% protein, and 5-10% carbohydrates. For insulin-dependent individuals, protein intake must be precise; excessive amounts can trigger gluconeogenesis, raising blood sugar. A safe range is 1.2-1.5 grams of protein per kilogram of body weight daily. For instance, a 70 kg (154 lb) person should consume 84-105 grams of protein. Carbohydrates should be limited to 20-30 grams daily, focusing on fiber-rich sources like leafy greens and berries to stabilize glucose levels.
Micronutrient deficiencies are a hidden risk for diabetics on keto. The restrictive nature of the diet can lead to inadequate intake of B vitamins, particularly thiamine and folate, which are crucial for nerve function and blood sugar regulation. Supplementation or inclusion of keto-friendly foods like almonds, seeds, and low-carb vegetables can mitigate this. Additionally, omega-3 fatty acids from sources like fatty fish or flaxseeds are essential to reduce inflammation, a common concern in diabetes. Regular blood tests to monitor nutrient levels are advisable.
Practical implementation requires a structured approach. Start by tracking daily nutrient intake using apps like MyFitnessPal or Cronometer, ensuring macronutrient ratios align with keto guidelines. Incorporate nutrient-dense foods like eggs, fatty fish, and olive oil to meet fat requirements while avoiding processed fats. For electrolytes, add a pinch of salt to meals or drink bone broth. Consult a dietitian to tailor the plan to individual needs, especially for those on insulin therapy, as dosage adjustments may be necessary. Consistency and vigilance are key to safely navigating the keto diet as an insulin-dependent diabetic.
Is Ponzu Sauce Keto-Friendly? A Low-Carb Diet Guide
You may want to see also
Frequently asked questions
Yes, insulin-dependent diabetics can follow a keto diet, but it requires careful monitoring and close collaboration with a healthcare provider to adjust insulin doses and manage blood sugar levels.
A keto diet typically reduces carbohydrate intake, which can lower blood sugar levels. However, insulin doses may need to be adjusted to prevent hypoglycemia (low blood sugar).
Risks include hypoglycemia, ketoacidosis (if insulin is insufficient), and electrolyte imbalances. Regular monitoring and medical supervision are essential to mitigate these risks.
Yes, insulin doses often need to be reduced on a keto diet due to lower carbohydrate intake. Failure to adjust doses can lead to dangerously low blood sugar levels.
Some studies suggest a keto diet may improve insulin sensitivity over time, but individual responses vary. It’s important to monitor progress and consult a healthcare provider for personalized advice.