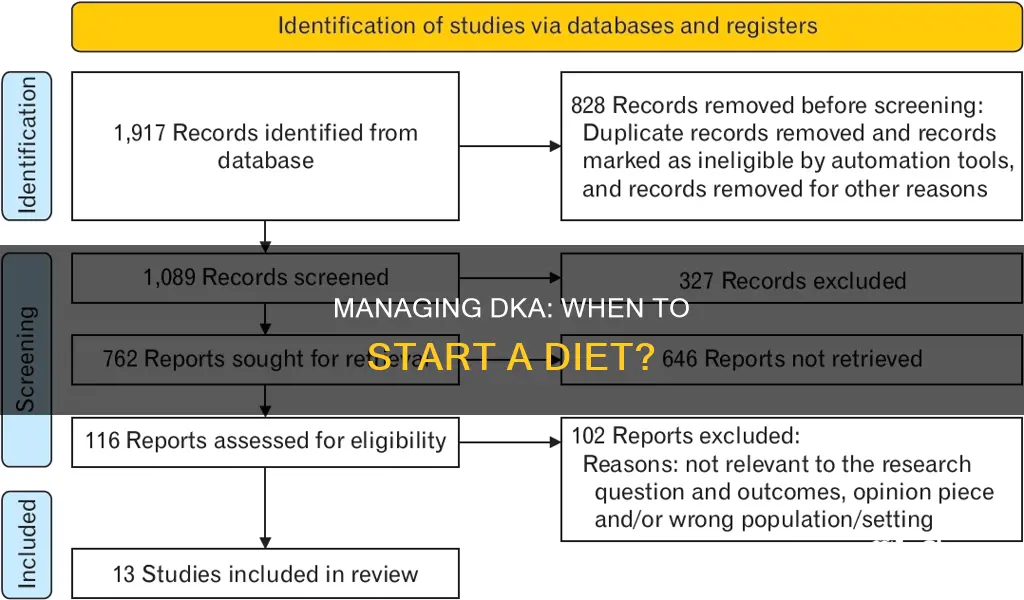
Diabetic ketoacidosis (DKA) is a serious and potentially fatal complication of diabetes, requiring immediate medical attention. It occurs when the body does not produce enough insulin, leading to a breakdown of body fat for energy and a subsequent release of ketones into the bloodstream. This results in high blood sugar levels and can cause severe insulin deficiency, electrolyte abnormalities, and dehydration. If left untreated, DKA can lead to death. While there is no consensus on the optimal timing for initiating oral nutrition in DKA patients, studies suggest that early nutrition within the first 24 hours of admission is safe and may lead to shorter hospital stays. Managing DKA involves controlling blood sugar levels, rehydration, and transitioning to subcutaneous insulin and oral nutrition.
| Characteristics | Values |
|---|---|
| When to start a diet in DKA | There is no consensus on the appropriate timing for initiating oral nutrition in patients with diabetic ketoacidosis (DKA). However, studies suggest that starting oral nutrition within the first 24 hours of admission to a medical intensive care unit (MICU) is safe and results in shorter intensive care unit and hospital stays. |
| Factors affecting the timing of oral nutrition in DKA | - Variability among physicians: There is existing variability among physicians regarding the optimal timing of initiating oral nutrition in patients with DKA. |
| - Patient demand: Elevated ketone bodies and free fatty acid (FFA) levels, which can suppress hunger, may contribute to the delay in oral intake when initiated upon the patient's demand. | |
| Dietary considerations for DKA prevention | - Good blood sugar control: Maintaining target blood sugar levels through diet, exercise, and medications can help prevent DKA. |
| - Meal planning: Following a meal plan and avoiding low-carbohydrate diets can help manage diabetes and prevent ketosis, a precursor to DKA. |
Explore related products




What You'll Learn
![]()
DKA patients' oral nutrition within 24 hours of admission
Diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes that requires immediate medical attention. It occurs when the body does not have enough insulin, leading to a breakdown of body fat for energy, which results in a high number of ketones in the blood and causing the blood to become acidic.
Upon admission, DKA patients require insulin infusion and careful monitoring of their electrolyte and blood sugar levels. However, there is no consensus on the appropriate timing for introducing oral nutrition, and practices vary among physicians. While some advocate for early nutrition within the first 24 hours of admission, others recommend a late nutrition approach, providing oral nutrition after the initial 24-hour period.
Studies have shown that early oral nutrition for DKA patients within 24 hours of admission is safe and does not increase the rate of DKA complications. It is associated with shorter intensive care unit (ICU) and hospital stays. Early nutrition may also contribute to faster DKA resolution and anion gap normalization, although these findings were not statistically significant in one study.
On the other hand, potential disadvantages of early oral nutrition within 24 hours include challenges in blood sugar monitoring and insulin dosing, altered mental status leading to aspiration risks, and worsening nausea, vomiting, and abdominal pain. These concerns have led many institutions to adopt different protocols for initiating oral nutrition.
In conclusion, while there is no definitive guideline, early oral nutrition for DKA patients within 24 hours of admission appears safe and may offer benefits in terms of reducing hospital and ICU length of stay. However, medical professionals must carefully consider the potential disadvantages and closely monitor patients to ensure their safety.
Cranberry Juice: Healthy Drink or Sugar Trap?
You may want to see also
Explore related products






![]()
Oral nutrition after 24 hours of admission
Diabetic ketoacidosis (DKA) is a serious and potentially life-threatening complication of diabetes that occurs when the body does not have enough insulin, a hormone that is essential for turning glucose (sugar) into energy. In the absence of sufficient insulin, the body starts breaking down fat for energy, leading to a buildup of ketones in the bloodstream and resulting in blood acidity or ketoacidosis.
The early signs of DKA include frequent urination, extreme thirst, and intense hunger. If left untreated, DKA can be fatal, with a mortality rate of 1% to 5%. However, with appropriate treatment, the survival rate exceeds 95%. Treatment for DKA typically involves insulin infusion, close monitoring of electrolyte and blood sugar levels, and subsequent transition to subcutaneous insulin and oral nutrition.
While there are no established guidelines regarding the optimal timing for initiating oral nutrition in DKA patients, studies have compared the outcomes of early nutrition (within the first 24 hours of admission) and late nutrition (after the first 24 hours). Results suggest that early oral nutrition is safe and associated with shorter intensive care unit and hospital stays. However, it is important to note that the delay in oral diet resumption in the late nutrition group may have contributed to the delayed transfer of patients out of the intensive care unit.
In conclusion, although there is no consensus on the exact timing, initiating oral nutrition within the first 24 hours of admission for DKA patients appears to be beneficial in terms of reducing hospital stay duration without increasing the risk of complications.
Vitamin E: Easy Ways to Add to Your Daily Diet
You may want to see also
Explore related products


![]()
Insulin infusion and monitoring of electrolytes and blood sugar
Diabetic ketoacidosis (DKA) is a medical emergency caused by a severe insulin deficiency. It is a potentially fatal complication of diabetes that requires immediate treatment. The goals of DKA treatment are to normalize fluid-volume status, hyperglycemia, electrolytes, and ketoacidosis.
Insulin therapy is a critical component of DKA treatment. The recommended insulin regimens include an initial IV bolus of regular insulin, followed by continuous insulin infusion at a specific rate. The 2011 JBDS guideline recommends weight-based fixed-rate intravenous insulin infusion until ketosis subsides. If blood sugar falls below a certain threshold, glucose should be added to allow for the continuation of insulin infusion.
In established patients with diabetes, long-acting insulin should be initiated at the dose previously used. However, for patients with newly diagnosed diabetes, smaller doses are generally recommended to avoid hypoglycemia. The SQuID protocol is specifically designed for managing mild-to-moderate DKA with subcutaneous insulin alone.
Monitoring of electrolytes and blood sugar levels is crucial during DKA treatment. Frequent blood glucose monitoring helps identify and manage DKA early on. Electrolyte abnormalities, such as hypokalemia and hyperkalemia, can complicate DKA treatment. Aggressive monitoring and treatment of electrolyte imbalances are necessary to optimize insulin therapy and patient outcomes.
Overall, insulin infusion and the careful monitoring of electrolytes and blood sugar levels are essential components of DKA management. The specific insulin regimens and monitoring protocols ensure patient stability and the effective resolution of DKA.
Diets in European History: Their Significance and Legacy
You may want to see also
![]()
Oral diet resumption delay
Diabetic ketoacidosis (DKA) is a serious and potentially fatal complication of diabetes. It occurs when the body does not have enough insulin, a hormone that is essential for converting glucose (blood sugar) into energy. In the absence of sufficient insulin, the body starts breaking down fat for energy, leading to a buildup of ketones in the bloodstream, which causes the blood to become too acidic.
The early signs of DKA include frequent urination, extreme thirst, and intense hunger. If left untreated, DKA can be life-threatening, with a mortality rate of 1% to 5%. Treatment for DKA involves insulin infusion, close monitoring of electrolyte and blood sugar levels, and subsequent transition to subcutaneous insulin and oral nutrition.
There is no consensus or guideline on the appropriate timing for the initiation of oral nutrition in patients with DKA. Some studies have compared the outcomes of early nutrition (within the first 24 hours of admission) and late nutrition (after the first 24 hours of admission). While patients in the late nutrition group experienced a delay in DKA resolution and anion gap normalization, neither difference was found to be statistically significant.
However, it is important to note that oral diet resumption delay may contribute to prolonged stays in the intensive care unit. This delay could be attributed to the suppressive effect of higher ketone levels on hunger, which is often observed in patients with DKA. Therefore, while the timing of oral nutrition initiation may not significantly impact DKA resolution, it could have implications for the length of hospital stays and patient management.
Protein Deficiency: Understanding the Impact and Health Risks
You may want to see also
![]()
Factors affecting mortality rates
Diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes, with an associated mortality rate of 1% to 5%. However, with appropriate treatment, the survival rate is over 95%. Here are some factors that can affect mortality rates in individuals with DKA:
Age: Older age is a risk factor for higher mortality rates in individuals with DKA. Specifically, DKA hospitalization rates are significantly higher among individuals under 45, and the incidence of DKA is highest during adolescence for those with type 1 diabetes. However, DKA in elderly individuals is also associated with high mortality rates.
Type of Diabetes: While DKA is more common in individuals with type 1 diabetes, it also occurs in those with type 2 diabetes. Studies have shown that DKA is more severe and associated with higher mortality rates in patients with type 2 diabetes.
Socioeconomic Status: Individuals from disadvantaged socioeconomic backgrounds have higher incidence rates of DKA. Risk factors include low socioeconomic status, low education, and low adherence to therapy.
Comorbidities: Certain comorbidities and conditions increase the risk of mortality in individuals with DKA. These include sepsis, obesity, and a higher Charlson comorbidity index. Additionally, having coexisting acute conditions, such as a heart attack, pneumonia, or sepsis, can lead to worse outcomes.
Bacteremia: The presence of bacteremia, as indicated by positive blood cultures, is associated with increased mortality rates in DKA patients. The mortality rates of those with bacteremia were significantly higher than those without.
Other Factors: Other factors that can affect mortality rates include brain swelling, especially in younger individuals, and receiving treatment after falling into a coma. Delayed initiation of oral nutrition in DKA patients may also contribute to delayed transfer out of the intensive care unit, potentially impacting mortality rates.
Rebel Wilson's Weight Loss Journey: Her Diet Plan Revealed
You may want to see also
Frequently asked questions
Diabetic ketoacidosis (DKA) is a serious and potentially fatal complication of diabetes that occurs when the body doesn't produce enough insulin, a hormone that turns glucose into energy. This causes the body to break down fat for energy, leading to a high level of ketones in the blood and making the blood too acidic.
Early signs of DKA include frequent urination, extreme thirst, intense hunger, frequent vomiting, tiredness, and difficulty breathing.
DKA is a medical emergency. If you think you have DKA, seek immediate medical attention.
Treatment for DKA typically involves insulin infusion, close monitoring of electrolyte and blood sugar levels, and transitioning to subcutaneous insulin and oral nutrition. Good blood sugar control through diet, exercise, and medication can help prevent DKA.



















