Refeeding anorexia nervosa can be a challenging process, both physically and mentally. The refeeding process involves an individual increasing their caloric intake after a period of consuming very little food, which can be overwhelming for those with anorexia. It is important to be aware of the potentially fatal refeeding syndrome, which can cause serious complications due to sudden shifts in fluids and electrolytes. This can be prevented by careful management of the refeeding process, which should be overseen by a medical team. The recovery process can be long, and patients often require substantial emotional support and motivation to increase their caloric intake.
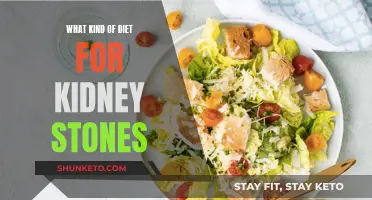
Diet for refeeding anorexia
| Characteristics | Values |
|---|---|
| Caloric intake | 3,000 to 5,000 calories per day |
| Weight gain | 1/2 pound to 2 pounds per week |
| Meal plan | Three 500- to 800-calorie meals and three 300-calorie snacks |
| Macronutrient proportions | 50–60% of total calories from carbohydrates, 15–20% from protein, and 30–40% from dietary fat |
| Refeeding syndrome prevention | Electrolyte replacement before receiving food, reducing caloric intake while introducing electrolytes |
| Medical team | Medical doctor, registered dietitian nutritionist, psychotherapist, psychiatrist |
| Exercise | Should be restricted at the start of the refeeding process due to potential deficiencies in electrolytes and minerals |
| Fibre intake | Should be limited at the start of the refeeding process to reduce digestive discomfort |
Explore related products





What You'll Learn
![]()
The role of a dietitian in anorexia recovery
Anorexia nervosa is a psychiatric disorder that affects both physical and mental health. Treatment for anorexia often involves a multidisciplinary team, including a medical doctor, a registered dietitian nutritionist, a psychotherapist, and a psychiatrist. Dietitians are a valuable resource in the treatment of anorexia nervosa, and their role is to help patients establish a foundation for long-term recovery.
Registered dietitians tailor recommendations to the individual, taking into account their specific calorie needs, which shift during the recovery process. They also provide emotional support and motivation to help patients increase their oral intake to a caloric amount that supports consistent weight restoration. The preferred meal plan model for anorexia nervosa recovery is the exchange system, which considers macronutrient proportions (protein, carbohydrates, and fat) without directly focusing on calories.
In the context of family therapy for anorexia nervosa (FT-AN), dietitians are considered a core member of the treating team. Dietetic involvement is particularly valuable during the initial phases of treatment, where nutritional rehabilitation typically occurs, and in atypical cases with healthy weights or co-morbid complexities. Dietitians collaborate with other clinicians to create treatment guidelines that incorporate diverse perspectives and address the medical, psychological, and nutritional aspects of anorexia nervosa.
It is important to be aware of refeeding syndrome, which can occur when someone in a state of starvation suddenly consumes a large amount of food. This can lead to electrolyte imbalances and issues with muscles, lungs, heart, and brain function, resulting in swelling, confusion, and even death. To prevent refeeding syndrome, doctors may recommend reducing caloric intake while introducing electrolytes through nutrient-dense solutions before providing food.
Calorie Counting on the Mediterranean Diet: Is It Necessary?
You may want to see also
Explore related products


$29.95 $23.95




![]()
How to avoid refeeding syndrome
Refeeding syndrome is a potentially fatal condition that can occur when someone who has been malnourished consumes a large amount of food at once. The condition involves a sudden shift in fluid and electrolyte levels, which can lead to swelling, confusion, and even death. It is often associated with anorexia nervosa, but it can also occur in people with other medical conditions or those who have faced starvation for prolonged periods.
- Slow and gradual refeeding: Start with a low caloric intake and slowly increase it over time. For patients at high risk of developing refeeding syndrome, nutritional repletion should be started slowly (maximum 0.042 MJ/kg/24 hours) and tailored to each patient. It can then be gradually increased to meet full needs over four to seven days. This is especially important for individuals with severe eating disorders or malnutrition, as they are at high risk for refeeding syndrome.
- Correct electrolyte and fluid imbalances: Before initiating refeeding, it is crucial to correct any electrolyte and fluid imbalances. Electrolyte replacement can be done by providing patients with nutrient-dense solutions for up to three days before introducing food. Electrolyte levels should be monitored closely during the refeeding process, with daily measurements in the first week and at least three times in the second week.
- Vitamin supplementation: Start vitamin supplementation immediately, both before and during the first 10 days of refeeding. This includes oral, enteral, or intravenous supplements of potassium, phosphate, calcium, and magnesium, unless blood levels are high before refeeding.
- Cardiorespiratory monitoring: Patients at high risk of cardiac complications should undergo cardiorespiratory monitoring. This includes monitoring of cardiac rhythm and central venous pressure.
- Individualized approach: Nutritional rehabilitation should be individualized, with input from a registered dietitian and other clinical team members specializing in malnutrition and eating disorders. A meal plan should be carefully constructed, taking into account the patient's specific needs and the potential for triggering anxiety associated with calorie-focused plans.
- Early detection: Be vigilant for early signs and symptoms of refeeding syndrome, such as lab abnormalities like thiamin deficiency (vitamin B1), elevated creatine phosphokinase (CPK), and acute worsening of anemia. Detecting these early indicators can help prevent further complications.
- Psychological support: The cognitive and emotional aspects of refeeding in patients with anorexia nervosa must be addressed. Patients often require substantial emotional support and motivation during the refeeding process. Incorporating psychological or therapeutic techniques can help encourage progress and promote healing.
Tuna Troubles: HCG Diet Restrictions and Why
You may want to see also
Explore related products






![]()
Meal plans for anorexia recovery
Meal plans are an important part of anorexia recovery, but they should be approached with caution. The body of a person recovering from anorexia is malnourished and in a state of starvation, so it is important to be aware of the potentially fatal refeeding syndrome. This occurs when the body suddenly switches from using fat and protein to carbohydrates as its primary source of energy, causing a sudden shift in fluid and electrolytes that can lead to serious and dangerous complications.
A treatment team for anorexia nervosa should include a medical doctor, a registered dietitian nutritionist, a psychotherapist, and a psychiatrist. A registered dietitian will create a meal plan for an individual’s specific needs, providing structure, supporting nutritional needs, and establishing healthy eating patterns. This plan will be tailored to the individual, taking into account their specific calorie needs, which will change as they gain weight. The dietitian will also incorporate psychological or therapeutic techniques to encourage the patient’s progress and provide education to promote long-term successful outcomes.
The preferred meal plan model for anorexia nervosa recovery is the exchange system, which considers macronutrient proportions (protein, carbohydrates, fat) without directly focusing on calories. Calculations often aim to reach 50–60% of total calories from carbohydrates, 15–20% from protein, and 30–40% from dietary fat for metabolic efficiency. Each “exchange” (starch, fruit, vegetable, milk, fat, protein/meat) equates to a certain food and its portion size. This allows for a focus on balanced food group selection during meal planning.
A good initial rule of thumb for a basic meal plan is three 500- to 800-calorie meals plus at least three 300-calorie snacks, but only after initial caloric estimates are calculated and monitored and the refeeding syndrome has been ruled out. For adolescents, this can be safely started at an intake of 2,000 to 2,500 calories per day, increasing to 3,000 to 5,000 calories per day for weight restoration.
Wine and Starch Diet: What's the Verdict?
You may want to see also
Explore related products






![]()
The importance of addressing the psychological aspects of anorexia
Anorexia nervosa is a complex psychiatric condition with a high mortality rate. It is characterised by a distorted body image and a preoccupation with food and weight. Those with anorexia often have a deep fear of gaining weight and see themselves as bulky or fat. This distorted belief leads to severely restricted food intake and other problematic eating patterns, such as binge eating, purging, and the abuse of laxatives. The condition can have severe physical consequences, including malnutrition, cardiac problems, and infertility. It can also lead to depression, relationship difficulties, and even suicide.
The treatment of anorexia nervosa requires a comprehensive approach that addresses both the physical and psychological aspects of the disorder. While nutritional rehabilitation is crucial, it is equally important to address the underlying psychological issues that contribute to and result from the condition. This includes helping the person recognise and accept that they have a serious disorder, as many people with anorexia deny that they have an eating disorder. Cognitive behavioural therapy (CBT) is often used to address distorted views and attitudes about weight, shape, and appearance, and to encourage behavioural changes. Other therapeutic approaches, such as cognitive remediation therapy, dialectical behaviour therapy (DBT), and interpersonal psychotherapy (IPT), can also be beneficial in improving relationships, managing emotions, and addressing the root causes of the disorder.
The support of a registered dietitian is crucial in initiating and advancing meal plans for weight restoration, monitoring weight trends, and providing nutrition education. However, due to the psychological complexities of anorexia, it is important for dietitians to incorporate psychological or therapeutic techniques into their practice. This may include providing emotional support and motivation to help patients increase their oral intake to a sufficient caloric amount and encouraging the development of a healthier relationship with food.
Additionally, addressing the psychological aspects of anorexia is crucial in preventing relapse and promoting long-term recovery. This includes helping patients develop a more positive body image and improving their self-esteem. Family support is also an important aspect of treatment, as family members can provide ongoing encouragement and understanding of the disorder. Overall, the treatment of anorexia nervosa requires a multidisciplinary approach that addresses the physical, psychological, and social needs of the individual.
The Benefits of Green Salad on the HCG Diet
You may want to see also
Explore related products






![]()
The impact of anorexia on the body
Anorexia Nervosa is a severe eating disorder that can have detrimental effects on the body and mind. The disorder is characterised by a distorted body image and an intense fear of weight gain, leading to a refusal to maintain a healthy body weight. The impact of anorexia on the body can be severe and wide-ranging, affecting multiple organs and systems.
One of the key consequences of anorexia is malnutrition, which can cause hair loss, skin and nail changes, and a reduction in bone density. This is due to the body's decreased energy expenditure during starvation, resulting in reduced energy allocation to bone maintenance. Studies indicate that a large proportion of individuals with anorexia have either osteoporosis or osteopenia, putting them at significant risk of bone fractures.
Anorexia can also lead to gastroparesis, which is a delayed emptying of the stomach. This results in bloating, upper stomach pain, constipation, and infrequent bowel movements. Purging behaviours associated with anorexia, such as vomiting or laxative misuse, can have additional consequences such as tooth enamel erosion, esophageal tears, and colon muscle damage.
The restriction of food and excessive exercise common in anorexia can deplete glycogen stores, leading to abnormal glucose metabolism and hypoglycaemia. As starvation progresses, blood flow slows down, causing intolerance to cold temperatures and a bluish tint in the extremities. The body may produce lanugo hair, fine hair that grows on the face and body, in an attempt to retain body heat.
Anorexia can also have severe effects on the brain, which are reversible with proper treatment. Individuals with anorexia may experience changes in their mental health and cognitive function due to the lack of nutrients. Additionally, the condition can impact the respiratory and cardiovascular systems, with potential long-term consequences.
The process of refeeding individuals with anorexia must be carefully managed to prevent refeeding syndrome, which can be life-threatening. This syndrome involves a sudden shift in fluids and electrolytes, leading to complications in the muscles, lungs, heart, and brain. A medical team, including a doctor, dietitian nutritionist, psychotherapist, and psychiatrist, typically oversees the refeeding process and provides emotional support to help individuals increase their caloric intake gradually.
Dash Diet: Can It Help Fight Hereditary Hypertension?
You may want to see also
Frequently asked questions
Refeeding syndrome is a series of symptoms that can occur when an individual has been malnourished for a long time and then reintroduces too many calories to their diet too quickly. It is characterised by fluid and electrolyte imbalances, changes in metabolism, and changes in levels of phosphate, potassium, and magnesium in the body. Refeeding syndrome can lead to serious complications and even death.
Symptoms of refeeding syndrome include swelling, confusion, nausea, vomiting, muscle weakness, trouble breathing, double vision, swallowing problems, and constipation. It can also lead to heart and kidney failure, as well as respiratory failure.
Refeeding syndrome can be prevented by gradually increasing caloric intake and monitoring weight gain. It is important to work with a medical team, including a doctor, dietitian, and therapist, to ensure a safe and effective refeeding process. Electrolyte replacement before receiving food can also help prevent refeeding syndrome.
Some tips for the refeeding process include restricting exercise at the beginning, limiting dietary fibre intake initially, and providing emotional support and motivation to increase oral intake. It is important to address any electrolyte and mineral deficiencies before reintroducing exercise, and to be aware of potential digestive discomfort during the early stages of refeeding.