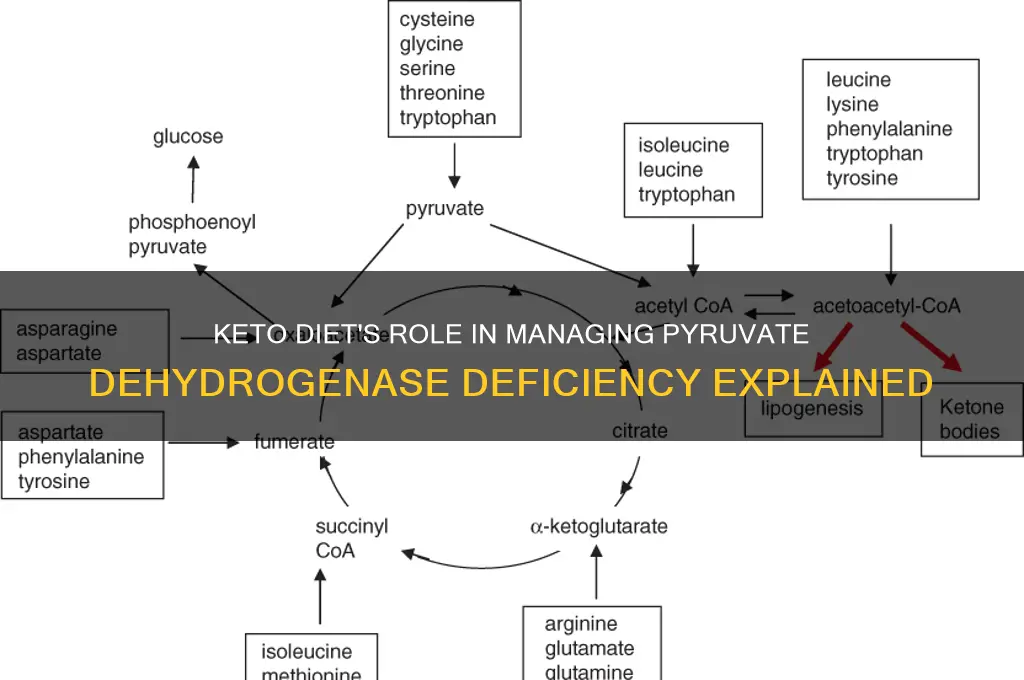
Pyruvate dehydrogenase deficiency (PDHD) is a rare metabolic disorder characterized by impaired activity of the pyruvate dehydrogenase complex (PDC), which plays a critical role in converting glucose into energy via the citric acid cycle. Individuals with PDHD often experience neurological symptoms and lactic acidosis due to the accumulation of pyruvate and lactate. A ketogenic diet, which is high in fats and low in carbohydrates, has emerged as a therapeutic approach for managing PDHD. By minimizing carbohydrate intake, the diet reduces the reliance on glucose metabolism, thereby decreasing the workload on the compromised PDC. Instead, the body shifts to utilizing ketone bodies, derived from fat metabolism, as an alternative energy source. This metabolic shift not only alleviates the buildup of toxic metabolites like lactate but also provides a more efficient energy supply for the brain, potentially mitigating neurological symptoms and improving overall function in individuals with PDHD.
| Characteristics | Values |
|---|---|
| Mechanism of Keto Diet | Provides ketone bodies (β-hydroxybutyrate, acetoacetate) as alternative energy source. |
| Bypass Pyruvate Dehydrogenase Complex (PDC) | Ketone bodies bypass the blocked PDC pathway, reducing reliance on glucose metabolism. |
| Reduced Pyruvate Accumulation | Decreases pyruvate buildup, alleviating symptoms of lactic acidosis. |
| Improved Energy Production | Ketones serve as efficient fuel for the brain and muscles, compensating for impaired glucose oxidation. |
| Decreased Lactic Acid Production | Reduces lactic acid formation, which is a byproduct of impaired PDC function. |
| Neuroprotective Effects | Ketones provide neuroprotection and stabilize brain energy metabolism. |
| Symptom Management | Improves neurological symptoms, fatigue, and cognitive function in PDC deficiency. |
| Long-Term Metabolic Support | Sustains energy needs without overburdening the defective PDC pathway. |
| Clinical Evidence | Supported by case studies and anecdotal evidence in PDC deficiency patients. |
| Dietary Implementation | High-fat, low-carbohydrate diet to maintain ketosis. |
Explore related products

$13.46 $21.99





What You'll Learn
- Ketone Bodies as Alternative Fuel: Ketones bypass PDH, providing energy without relying on dysfunctional pyruvate dehydrogenase complex
- Reduced Glucose Dependence: Lower carb intake minimizes pyruvate accumulation, easing metabolic stress on deficient PDH
- Decreased Lactate Production: Keto reduces glycolysis, lowering lactate levels and associated metabolic acidosis risks
- Improved Mitochondrial Function: Ketones enhance mitochondrial efficiency, compensating for PDH deficiency-related energy deficits
- Neuroprotective Effects: Ketones stabilize brain energy metabolism, mitigating neurological symptoms linked to PDH deficiency
![]()
Ketone Bodies as Alternative Fuel: Ketones bypass PDH, providing energy without relying on dysfunctional pyruvate dehydrogenase complex
Pyruvate dehydrogenase deficiency (PDHD) disrupts the body's ability to convert glucose into energy, leaving individuals reliant on alternative fuel sources. Ketone bodies, produced during ketosis, emerge as a critical workaround. Unlike glucose, ketones bypass the dysfunctional pyruvate dehydrogenase complex (PDC), entering the mitochondria independently to fuel cellular respiration. This metabolic detour restores energy production, alleviating symptoms like lethargy, cognitive impairment, and lactic acidosis associated with PDHD.
Consider the biochemical pathway: during ketosis, fatty acids are broken down into acetoacetate, beta-hydroxybutyrate, and acetone—collectively known as ketone bodies. These molecules cross the mitochondrial membrane without PDC involvement, directly entering the citric acid cycle as acetyl-CoA. For PDHD patients, this means energy generation can continue even when glucose metabolism is impaired. Clinical studies suggest that maintaining serum ketone levels between 1-3 mmol/L can significantly improve energy availability and reduce disease severity.
Implementing a ketogenic diet to achieve this requires precision. Typically, dietary macronutrients should consist of 70-80% fat, 15-20% protein, and 5-10% carbohydrates. For children with PDHD, this often translates to 3-4 grams of fat per kilogram of body weight daily, adjusted based on age and metabolic needs. Adults may require higher fat intake, monitored via ketone testing strips or blood meters to ensure therapeutic levels. Caution is advised for individuals with renal or hepatic issues, as ketosis can exacerbate these conditions.
A comparative analysis highlights the ketogenic diet’s superiority over glucose-dependent therapies in PDHD management. While high-carbohydrate diets worsen PDC overload and lactic acidosis, ketosis provides a sustainable, PDC-independent energy source. However, adherence challenges—such as palatability and long-term compliance—necessitate multidisciplinary support, including dietitians and physicians. Emerging research also explores exogenous ketone supplements as a complementary strategy, though their efficacy in PDHD remains under investigation.
In practice, caregivers and patients must prioritize consistency and monitoring. Gradual dietary transitions, regular biochemical assessments, and symptom tracking are essential. For instance, sudden drops in ketone levels may indicate dietary lapses or metabolic shifts, requiring immediate adjustments. While the ketogenic diet is not a cure for PDHD, its ability to harness ketone bodies as alternative fuel offers a transformative approach to managing this rare metabolic disorder.
Is Butternut Squash Keto-Friendly? A Low-Carb Diet Guide
You may want to see also
Explore related products






![]()
Reduced Glucose Dependence: Lower carb intake minimizes pyruvate accumulation, easing metabolic stress on deficient PDH
Pyruvate dehydrogenase deficiency (PDHD) is a rare metabolic disorder where the body struggles to convert pyruvate, a byproduct of glucose metabolism, into acetyl-CoA, a crucial molecule for energy production. This inefficiency leads to a buildup of pyruvate, causing metabolic stress and symptoms like lactic acidosis, neurological impairment, and developmental delays. A ketogenic diet, characterized by high fat, moderate protein, and very low carbohydrate intake, offers a strategic approach to alleviate this stress by fundamentally altering the body’s fuel source.
By drastically reducing carbohydrate intake, typically to less than 50 grams per day, the ketogenic diet minimizes glucose availability. This reduction directly lowers pyruvate production, as glucose is the primary substrate for glycolysis, the metabolic pathway that generates pyruvate. With less pyruvate accumulating, the deficient pyruvate dehydrogenase (PDH) enzyme is under less pressure to process it, reducing the metabolic burden on the system. For individuals with PDHD, this shift can mitigate symptoms and improve overall metabolic function.
The mechanism behind this benefit lies in the body’s transition to ketone bodies as an alternative energy source. When carbohydrate intake is low, the liver converts fatty acids into ketones, which can cross the blood-brain barrier and provide energy for the brain and other tissues. This metabolic flexibility bypasses the need for PDH activity, as ketones enter the citric acid cycle directly as acetyl-CoA, bypassing the pyruvate bottleneck. For example, a study published in *Molecular Genetics and Metabolism* demonstrated that patients with PDHD experienced reduced lactic acidosis and improved neurological outcomes when following a ketogenic diet.
Implementing a ketogenic diet for PDHD requires careful planning and monitoring. Carbohydrate intake should be strictly limited, often to 5–10% of total daily calories, while fats should comprise 70–80% and protein 10–20%. It’s crucial to avoid hidden carbohydrates in processed foods and focus on whole, nutrient-dense sources like avocados, nuts, and leafy greens. Regular blood ketone and glucose monitoring ensures the diet remains effective, and adjustments may be necessary based on individual tolerance and response. Pediatric patients, in particular, may require additional supplementation with vitamins and minerals to support growth and development.
While the ketogenic diet is a powerful tool for managing PDHD, it is not without challenges. Adherence can be difficult, especially for children, and potential side effects include constipation, dehydration, and nutrient deficiencies. Long-term use requires ongoing medical supervision to address these issues and ensure the diet remains safe and effective. Despite these considerations, the reduction in glucose dependence and pyruvate accumulation makes the ketogenic diet a valuable therapeutic option for individuals with PDHD, offering a pathway to improved metabolic health and quality of life.
Should You Stop Keto? Understanding When and How to Transition Safely
You may want to see also
Explore related products

$8.32 $16.99
$21.45 $34.95

$14.85 $34.95



![]()
Decreased Lactate Production: Keto reduces glycolysis, lowering lactate levels and associated metabolic acidosis risks
Pyruvate dehydrogenase deficiency (PDHD) disrupts the body's ability to efficiently convert glucose into energy, leading to a reliance on alternative metabolic pathways. One consequence of this dysfunction is an over-reliance on glycolysis, the process of breaking down glucose for energy. This heightened glycolytic activity results in excessive lactate production, contributing to metabolic acidosis—a dangerous condition where the blood becomes too acidic. The ketogenic diet, by drastically reducing carbohydrate intake, directly addresses this issue by minimizing glycolysis and, consequently, lactate accumulation.
Consider the metabolic shift induced by a keto diet. Typically, carbohydrates are the primary fuel source, driving glycolysis and pyruvate production. In PDHD, pyruvate cannot be effectively converted to acetyl-CoA due to the enzyme deficiency, leading to a backlog of pyruvate and increased lactate formation. By limiting carbohydrate intake to less than 50 grams per day—a common keto guideline—the body transitions to using fats as the primary energy source. This shift not only bypasses the defective pyruvate dehydrogenase complex but also reduces the substrate available for glycolysis, thereby lowering lactate levels.
For individuals with PDHD, this reduction in lactate production is critical. Elevated lactate levels can lead to symptoms such as fatigue, muscle weakness, and, in severe cases, life-threatening metabolic acidosis. A well-formulated keto diet, rich in healthy fats (70-75% of daily calories), moderate in protein (20-25%), and low in carbohydrates, can mitigate these risks. Practical tips include incorporating foods like avocados, nuts, seeds, and fatty fish while avoiding high-carb staples like bread, pasta, and sugary snacks. Monitoring blood ketone levels (aiming for 0.5-3.0 mmol/L) ensures the body remains in ketosis, optimizing the metabolic shift away from glycolysis.
It’s important to note that while keto effectively reduces lactate production, it’s not a one-size-fits-all solution. Individual responses vary, and some may require additional interventions, such as supplementation with thiamine (a cofactor for pyruvate dehydrogenase) or carnitine (to support fatty acid oxidation). Pediatric cases, in particular, demand careful monitoring, as children with PDHD may have higher energy needs and are more susceptible to metabolic imbalances. Consulting a healthcare provider or dietitian to tailor the keto approach is essential for safety and efficacy.
In summary, the keto diet’s ability to decrease lactate production by reducing glycolysis offers a targeted strategy for managing PDHD-related metabolic acidosis. By minimizing carbohydrate intake and promoting ketosis, this dietary approach addresses the root cause of excessive lactate accumulation, providing a practical and evidence-based solution for individuals with this rare metabolic disorder.
Keto Diet and Lipedema: Exploring Potential Benefits and Limitations
You may want to see also
Explore related products






![]()
Improved Mitochondrial Function: Ketones enhance mitochondrial efficiency, compensating for PDH deficiency-related energy deficits
Ketones, the primary energy source on a ketogenic diet, bypass the need for pyruvate dehydrogenase (PDH) by fueling mitochondria through an alternative pathway. In individuals with PDH deficiency, glucose metabolism stalls at the pyruvate step, creating an energy bottleneck. Ketones, derived from fats, enter the mitochondria independently of PDH, directly feeding the citric acid cycle and ATP production. This metabolic detour restores energy supply, particularly to the brain and muscles, which are highly vulnerable to PDH-related deficits. For instance, medium-chain triglycerides (MCTs), a common ketogenic supplement, provide a rapid source of ketones, offering immediate relief from fatigue and cognitive fog in PDH-deficient patients.
The efficiency of ketone metabolism extends beyond mere energy substitution. Ketones produce more ATP per molecule compared to glucose, even in healthy individuals. This heightened efficiency becomes critical in PDH deficiency, where mitochondrial function is already compromised. Studies show that ketones reduce oxidative stress and enhance mitochondrial biogenesis, the process of creating new mitochondria. For practical application, a well-formulated ketogenic diet should aim for 70-80% fat, 15-20% protein, and 5-10% carbohydrates, ensuring sustained ketone production. Monitoring ketone levels (targeting 1-3 mmol/L) via blood or breath meters can optimize therapeutic benefits.
A comparative analysis highlights the ketogenic diet’s superiority over traditional high-carbohydrate diets for PDH deficiency. While carbohydrate restriction limits pyruvate accumulation, ketones actively improve mitochondrial resilience. This dual action not only compensates for energy deficits but also addresses the root cause of metabolic dysfunction. For children with PDH deficiency, early initiation of a ketogenic diet, often supplemented with MCT oil (starting at 0.5 g/kg/day and titrating up to 2 g/kg/day), has shown significant improvements in developmental milestones and seizure control. Adults may require higher fat intake, around 90% of daily calories, to achieve therapeutic ketosis.
Persuasively, the ketogenic diet’s role in PDH deficiency is not just palliative but potentially transformative. By shifting the body’s primary fuel source, it recalibrates mitochondrial function, offering a sustainable solution rather than a temporary fix. However, adherence is key. Practical tips include incorporating high-fat foods like avocados, nuts, and coconut oil, while avoiding hidden carbohydrates in processed foods. Regular follow-ups with a metabolic specialist are essential to monitor lipid profiles and adjust macronutrient ratios. For those hesitant about dietary restrictions, the long-term benefits—reduced fatigue, improved cognition, and enhanced quality of life—far outweigh the initial challenges.
Feeling Full on Keto: Understanding Satiety and Low-Carb Eating
You may want to see also
Explore related products






![]()
Neuroprotective Effects: Ketones stabilize brain energy metabolism, mitigating neurological symptoms linked to PDH deficiency
Ketones, produced during ketosis, serve as an alternative energy source for the brain when glucose utilization is impaired, as seen in pyruvate dehydrogenase (PDH) deficiency. This metabolic disorder disrupts the conversion of pyruvate to acetyl-CoA, limiting the brain’s primary fuel supply. By shifting the body into a state of ketosis through a keto diet, individuals with PDH deficiency can bypass this metabolic bottleneck. Ketones, derived from fatty acid breakdown, directly enter the mitochondrial citric acid cycle, providing a stable and efficient energy source for neuronal function. This metabolic adaptation is particularly critical for the brain, which relies heavily on continuous energy supply to maintain cognitive and motor functions.
The neuroprotective effects of ketones extend beyond energy provision. Ketones, such as beta-hydroxybutyrate (BHB), have been shown to modulate cellular signaling pathways that enhance neuronal resilience. For instance, BHB activates histone deacetylases (HDACs), which reduce oxidative stress and inflammation—common contributors to neurological decline in PDH deficiency. Additionally, ketones stabilize mitochondrial function by improving ATP production efficiency, even in the presence of impaired glucose metabolism. This dual role of ketones—as both an energy substrate and a signaling molecule—positions them as a potent therapeutic agent for mitigating neurological symptoms associated with PDH deficiency.
Implementing a keto diet for PDH deficiency requires careful consideration of macronutrient ratios and individual metabolic needs. A typical keto diet consists of 70–75% fat, 20–25% protein, and 5–10% carbohydrates, though these ratios may need adjustment based on age, severity of PDH deficiency, and clinical response. For children, who are more commonly affected by PDH deficiency, a modified keto diet with medium-chain triglycerides (MCTs) can be particularly beneficial. MCTs are rapidly converted to ketones, providing a quick and sustained energy source for developing brains. Monitoring ketone levels (targeting 1–3 mmol/L) and adjusting dietary intake accordingly ensures optimal therapeutic benefit without inducing metabolic imbalances.
Practical tips for adopting a keto diet in PDH deficiency include gradual carbohydrate reduction to minimize side effects like the "keto flu," incorporating nutrient-dense fats (e.g., avocados, nuts, and olive oil), and ensuring adequate hydration and electrolyte intake. Regular consultation with a metabolic specialist or dietitian is essential to tailor the diet to individual needs and monitor long-term outcomes. While the keto diet is not a cure for PDH deficiency, its ability to stabilize brain energy metabolism and mitigate neurological symptoms makes it a valuable component of comprehensive management strategies. By leveraging the neuroprotective effects of ketones, individuals with PDH deficiency can achieve improved quality of life and reduced disease burden.
Keto-Friendly Snacking: Delicious Low-Carb Options to Satisfy Your Cravings
You may want to see also
Frequently asked questions
Pyruvate dehydrogenase deficiency is a rare metabolic disorder where the body cannot properly convert glucose into energy due to a malfunctioning pyruvate dehydrogenase complex. The keto diet, which is high in fats and low in carbohydrates, bypasses the need for this complex by using ketones as an alternative energy source.
A keto diet minimizes carbohydrate intake, reducing the reliance on glucose metabolism. Since PDHD impairs the conversion of glucose to energy, lowering carbohydrate intake decreases the workload on the defective pyruvate dehydrogenase complex, alleviating symptoms and improving energy production.
Ketones, produced from fat breakdown during ketosis, serve as an alternative fuel source for the brain and muscles. This bypasses the defective pyruvate dehydrogenase pathway, providing energy without relying on glucose metabolism, which is compromised in PDHD.
While a keto diet can be beneficial for PDHD, it requires careful monitoring by a healthcare professional. Potential risks include nutrient deficiencies, electrolyte imbalances, and the need for individualized adjustments to ensure the diet meets specific metabolic needs. Regular medical supervision is essential.































